SOCIAL MEDIA
Portuguese Medical Association's Scientific Journal

Introduction: Over recent decades, brain resection for drug-resistant epilepsy has proven to be a valuable treatment option. The histopathological classification was of paramount value for patient management. The aims of this study were to characterize our resective epilepsy surgical series including the histopathological diagnoses and to understand the differences in clinical practice between two different periods of our epilepsy surgical programme.
Material and Methods: We performed a retrospective cohort study, including patients with drug-resistant epilepsy that underwent resective surgery between 1997 and 2021 in the Coimbra University Hospital Centre. Histopathological diagnoses were classified into seven major conventional categories. For comparison purposes, the cohort was divided into two consecutive periods of 12 years.
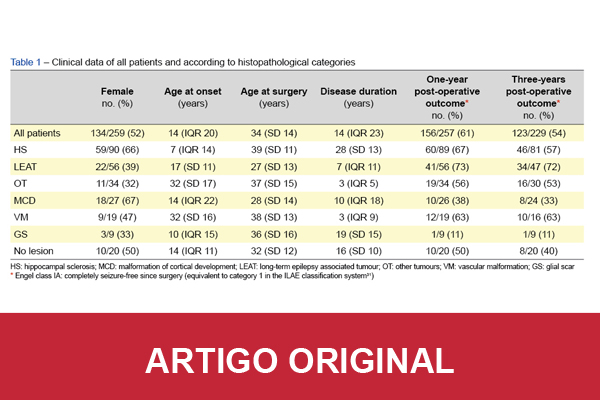
Results: A total of 259 patients were included, from which 228 (88%) were adults at the time of surgery. The median disease duration prior to surgery was 14 (interquartile range 23) years. Fifty-five (21%) patients performed pre-surgical invasive work-up. The temporal lobe was the most frequently operated region (73%). Major and minor post-surgical complications were identified in 21 (8%) patients. A reduction in the number of antiepileptic drugs was possible in 96 (37%) patients after surgery. The most common histopathological diagnosis was hippocampal sclerosis, but among children it was long-term epilepsy associated tumour. Long-term epilepsy associated tumours, hippocampal sclerosis and vascular malformations had the best post-operative outcomes. Malformations of cortical development and glial scars had the worst outcomes. Regarding differences between the two periods, the absolute number of operated patients increased (119 versus 140), and the age at surgery was higher in the second period (p = 0.04). The number of malformations of cortical development increased (p = 0.01), but the number of other tumours (p = 0.01) and specimens with no lesion (p = 0.03) decreased in the same period.
Conclusion: This study is in line with contemporaneous research, reinforcing the previous knowledge on the underlying structural aetiologies, clinical practice, and surgical outcomes over more than two decades of experience. Our data provide realistic expectations about epilepsy surgery and highlight the need for further improvements in diagnosis and treatment paradigm for people with chronic epilepsy.